Women's Pelvic Health

Pelvic floor dysfunction is common amongst women and can lead to a variety of symptoms. Examples of pelvic floor dysfunction include:
- Urinary frequency and urgency (needing to pass urine more often and rushing to pass urine)
- Urinary incontinence (bladder leaks)
- Pelvic organ prolapse
- Bowel incontinence (bowel leakage)
You can find out more in this leaflet: Lets talk about continence
The Pelvic Floor Muscles are a group of muscles that span the underside of your pelvis, forming the ‘floor’ of your pelvis. They insert into the pubic bone at the front, they fan out to the side into your sitting bones, and then into your tailbone/coccyx at the back.
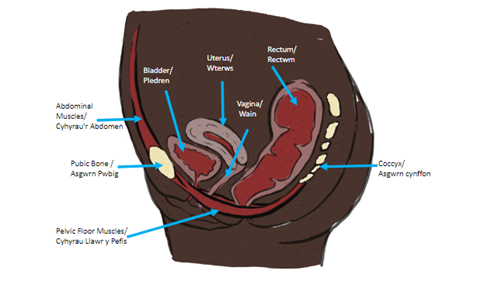
The Pelvic Floor Muscles support the bladder, reproductive organs, and bowels inside the pelvis, keep us continent of urine and faeces, provides stability to the spine and pelvis when we are active, and have an important role in sexual function.
The muscles can become dysfunctional (not work properly), this can be due to a number of factors including pregnancy and delivery, age, menopause, chronic choughs, chronic constipation. Typically, we think of pelvic floor muscles becoming weaker, with a reduction in endurance and function. This leads to symptoms such as urinary incontinence, pelvic organ prolapse and problems with bowel control.
If you think your muscles are weak follow the advice below.
How to find and exercise your pelvic floor muscles:
- Lie down or sit upright, in a comfortable position.
- Imagine that you are stopping yourself from passing wind and then stopping the flow of urine
- It should feel like a squeeze and lift up of the pelvic floor muscles from the back passage towards the bladder
- Other cues that can help engage your pelvic floor muscle include:
- Squeezing your pubic bone and your tail bone together
- Pretending you have a tail and curling it between your legs
- Imagine you are sucking up a marble with your back passage
- Continue to breath normally, don’t hold your breath or squeeze your buttocks or leg muscles, and ensure you fully relax after every squeeze
How often should we do them?
- Long squeezes - tighten up your pelvic floor muscles, hold the squeeze, then release/relax them fully. How long can you hold it for?
Repeat the long squeezes until the muscles fatigue. How many times can you repeat it?
Aim eventually to do 10 second holds and repeat 10 times
- Short Squeezes – quickly tighten up your pelvic floor muscles, then immediately release/relax them fully. How many times can you do this before the muscles fatigue?
Aim eventually to do these 10 times
- Repeat these exercises 3 times each day and try to do them in lie, sit or stand. Sitting or lying down will be easier to start with
- It is important to fully release/relax in between each squeeze. The aim is to have strong muscles that can fully lengthen too. ‘Pulsing’ your muscles could shorten them.
-
You may find it easier to start the exercises in lying or sitting but it is important to progress these to standing or functional positions where you feel you need more support from your pelvic floor muscles.
Further information and resources on Pelvic Floor Muscles can be found below:
This animation shows the location of your pelvic floor muscles – Pelvic Floor Anatomy
The following is a video and leaflet explaining pelvic floor muscle exercises further:
Squeezy: pelvic floor support app (squeezyapp.com)
Pelvic Floor Muscles and Breathing
It can be important to link your pelvic floor with your breath and having good breathing technique is important.
Very often, in day to day life we breathe shallowly mostly using our upper chest, rather than focusing on using our diaphragm.
Sit or lie comfortably with one hand lightly on your upper chest and one hand on your upper abdomen (tummy or belly), where it meets your lower ribs. Focus your attention on your breathing.
If comfortable for you, breathe in slowly through your nose, and then out through either your nose or mouth.
Aim to keep your upper chest more relaxed as you breathe in and out. You may need to adjust your position or posture so that the bottom of your ribcage can move freely. If you are slouched then the ribcage may be restricted.
Try imagining that you have a balloon in your abdomen and as you breathe in, the balloon is gently inflating with the breath. This should cause your tummy to gently rise, and your lower ribs to lift outwards. As you breathe out, imagine the balloon gently deflating – your abdomen should gently fall.
To link this with your pelvic floor exercises as you breathe out lift and squeeze your pelvic floor muscles holding as you take a few gentle breaths.
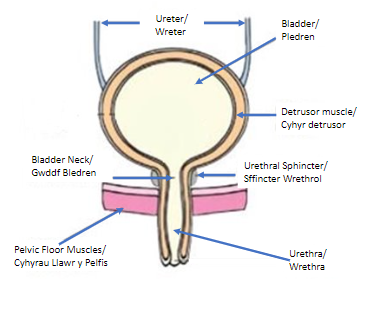
The kidneys filter our blood to remove excess water, waste, and produce urine, which travels along the ureters to the bladder. The bladder stores the urine and then empties it out.
We tend to get the initial desire to pass urine when it is holding approximately 150mls, but we often ignore these first signs. Generally, people visit the toilet to pass urine when it is convenient, and the bladder is holding approximately 400mls urine. This volume tends to be larger for the first void (wee) of the day.
A healthy bladder will need emptying up to 6-8 times per day, and not more than once during the night.
A healthy bladder should give us plenty of warning when it is getting full, be free of infections, and empty fully without pain or blood in our urine.
Aim to drink between 1.5 – 2 litres (6-8 mugs) daily.
You may want to avoid drinks that can irritate the bladder if you experience urinary frequency, urgency or urge incontinence.
Urinary incontinence is a common condition affecting 1 in 3 women. However, it should not be accepted as the norm and can improve with simple advice and exercises found below:
There are two main types of urinary incontinence:
Stress and urge incontinence can also occur together and this is known as mixed incontinence.
Bladder Frequency, urgency and urge incontinence may be due to an overactive bladder
If you are experiencing stress incontinence and/or urge incontinence strengthening your pelvic floor muscles can help to improve your symptoms – see the Pelvic floor exercises section for more information on this.
Healthy bladder habits
You may want to avoid drinks that can irritate the bladder if you experience urinary frequency, urgency or urge incontinence.
Bladder training
Bladder training can often help to reduce frequency, urgency and urge incontinence. This is explained in this leaflet - Bladder Training
Here is an example of a bladder diary (as described in the leaflet) that you can complete - Bladder Diary
If you have difficulty fully emptying your bladder, see the link below for helpful techniques
Pelvic floor dysfunction
Pelvic floor dysfunction can contribute to difficulties emptying the bladder. This can be due to either a weak or a tense pelvic floor. Assessment by a pelvic health physiotherapist will be able to guide you on whether your pelvic floor muscle needs strengthening or releasing if the above hasn't worked.
Bladder investigations
You may have been referred for investigations by your Consultant, Urology Nurse or Bladder and Bowel Nurse. The links below provide information regarding two common bladder tests:
Healthy bowel
Healthy bowel habits are important as straining to empty your bowels can make urinary incontinence worse, see the healthy bowel section for more advice.
Menopausal symptoms
Menopausal symptoms can influence pelvic floor dysfunction symptoms. See the menopause section for some useful information regarding the menopause.
Healthy Bowels should empty anything between 3 times per day and 3 times per week.
A stool (poo) should be easily passed without straining, pain, or blood.
It is important to avoid constipation and straining to empty your bowels as this can contribute to pelvic floor dysfunction.

Adjusting your position on the toilet

Drinking enough fluids

Eating plenty of fibre
All of the above can help, along with taking any medication prescribed for you. If you have difficulty emptying your bowels the section below has more information on this.
Constipation refers to infrequency or difficulty opening your bowels, where stools may be hard, lumpy or painful to pass.
Further information and tips for avoiding constipation can be found below:
- Constipation (NHS)
- Constipation (Guts UK)
- Fibre Fact Sheet (BDA)
- Tips to Encourage Healthy Bowel Habits
- Improving your Bowel Function - POGP
It is important that you regularly check your stools to rule out more serious conditions that can affect bowel function.
Key signs and symptoms to look out for can be found on the bowel cancer UK website - Bowel Cancer Symptoms
Adapting the position you use to sit on the toilet can help ‘straighten out’ the back passage, which makes it easier to pass stools. This sheet gives information about the best position to use - Correct Position for Emptying Bowels
The following videos may also be useful:
- How to avoid straining when going to the toilet my Physio SA Adelaide Physiotherapist (youtube.com)
- How To Open Your Bowels Without Straining (Michelle Kenway)
- 'I Love You' Abdominal Massage (ECO Physiotherapy)
It is also important to ensure you fully relax the pelvic floor when passing a stool, difficulty relaxing the pelvic floor can also contribute to problems with emptying.
The video below guides you through techniques to encourage relaxation of the pelvic floor whilst on the toilet:
Pelvic floor dysfunction can contribute to difficulties emptying the bowels. This can be due to either a weak or a tense pelvic floor. Assessment by a pelvic health physiotherapist will be able to guide you on whether your pelvic floor muscle needs strengthening or releasing if the above hasn't worked.
Menopausal symptoms can influence pelvic floor dysfunction symptoms. See the menopause section for some useful information regarding the menopause.
Bowel control problems can affect people in different ways:
- Sudden urges to poo that you can’t control
- Accidental bowel leakage
- Being unable to hold on to wind
The information below may be helpful:
Your pelvic floor muscles are responsible for controlling both your bladder and your bowels. Improving your pelvic floor strength can help to manage these symptoms. See the pelvic floor exercise section for further information on this.
Menopausal symptoms can influence pelvic floor dysfunction symptoms. See the menopause section for some useful information regarding the menopause.
The organs within a woman’s pelvis (uterus, bladder and rectum) are normally held in place by ligaments and muscles. If these support structures are weakened, the pelvic organs can bulge (prolapse) from their natural position into the vagina. When this happens it is known as pelvic organ prolapse. Sometimes a prolapse may be large enough to protrude outside the vagina
If you would like to see a drawing representing a prolapse please follow this link to the Royal College of Obstetrics and Gynaecology page Pelvic organ prolapse | RCOG
The POGP (Pelvic, Obstetric and Gynaecological Physiotherapy), a UK based Physiotherapy Professional Network affiliated to the Chartered Society of Physiotherapy have put together this leaflet explaining Pelvic Organ Prolapse and how to reduce the symptoms that you can read through here
Strengthening weak pelvic floor muscles can help to prevent or reduce pelvic organ prolapse symptoms. They can be strengthened by doing regular pelvic floor muscle exercises. See the pelvic floor exercise section for further information on this.
The POGP (Pelvic, Obstetric and Gynaecological Physiotherapy website contains useful information about using a pessary to manage prolapse symptoms.
Healthy bowel habits are important as straining to empty your bowels can make prolapse symptoms worse, see the healthy bowel section for more advice.
Some women find it helps to support the perineum (the area between the vagina and back passage) with a clean pad or toilet paper.
Menopausal symptoms can influence pelvic floor dysfunction symptoms. See the menopause section for some useful information regarding the menopause
 Pain during and/or after sex is known as dyspareunia - Dyspareunia – Pain with Intercourse
Pain during and/or after sex is known as dyspareunia - Dyspareunia – Pain with Intercourse
There are many causes of dyspareunia. Some women have tension in their pelvic floor muscles (sometimes known as an overactive or tight pelvic floor) and this may contribute to pain having sex. If you think you may have tension in your pelvic floor and would like to check, please see this information slide here
See below for some useful information that you may find helpful if you have an overactive or tight pelvic floor:
- Pelvic Floor Muscle Release Techniques
- Diaphragmatic Breathing
- Guided Visualization for Elimination (Constipation, Urinary Hesitancy, Incomplete Bladder Emptying)
- Pelvic Floor Release Stretches | FemFusion Fitness
- 3 Visualisations for Pelvic Floor Relaxation
- Guided Meditation for Pelvic Floor Relaxation
- Top 3 Pelvic Floor Stretches for Women and Men
- Easy Stretches to Relax the Pelvis
Vaginal dryness can be a cause of pain during intercourse. If you haven’t already, trying a natural lubricant can sometimes reduce this discomfort. There are a number of different types of lubricant including water based, oil based and silicone based. Please check the manufacturers instructions as some lubrications are not compatible with latex, silicone and other products. If you have tried these and are still having pain with intercourse, this is something Physiotherapy may be able to support you with.
Taking care of the vulval (genital area) skin is important - Care of Vulval Skin
This leaflet is useful if you have found having a smear test painful - Smears Without Tears
We see many women who have been referred to physiotherapy due to symptoms of persistent (also known as chronic) pelvic pain. These can include bladder pain syndrome (interstitial cystitis), chronic pelvic pain and vulvodynia:
See below for some useful information that you may find helpful if you have a persistent pain condition:
The ‘Education Programmes for Patients’ offer self-management health and wellbeing 6 week courses, including one focused on chronic pain. Participants need to self-refer (the form is on website below). The website also has some video relaxation sessions, and other resources.
See below for some useful information that you may find helpful if you have an overactive or tight pelvic floor:
- Pelvic Floor Muscle Release Techniques
- Diaphragmatic breathing
- Pelvic Floor Release Stretches | FemFusion Fitness
- 3 Visualisations for Pelvic Floor Relaxation
- Guided Meditation for Pelvic Floor Relaxation
- Top 3 Pelvic Floor Stretches for Women and Men
- Easy Stretches to Relax the Pelvis
Taking care of the vulval (genital area) skin is important - Care of Vulval Skin
This leaflet is useful if you have found having a smear test painful Smears without Tears
If you have endometriosis Endo Cymru has some useful information and you can also contact Endometriosis UK for support.
The Vulval Pain Society provides support for women with vulval pain.
Vaginismus is when the vagina suddenly tightens when trying to insert something in to it. Penetration of any kind may be difficult, painful or impossible. The term vaginismus refers to an involuntary contraction or spasm of the pelvic floor muscles surrounding the entrance to the vagina in response to attempted penetration. It is characterized by intense fear or anxiety related to vaginal penetration or intercourse.
Vaginismus doesn’t necessarily affect your ability to get aroused or enjoy sexual activity other than penetration.
Primary Vaginismus: This refers to a situation in which no form of vaginal penetration has ever been possible. It may be detected when first trying to use tampons, or first having penetrative sex.
Secondary Vaginismus: This refers to a situation in which pain-free penetration has been achieved previously and refers to a development of vaginismus symptoms at a later date.
Signs of Vaginismus can include:
- Difficulty inserting a tampon
- Burning or stinging pain with vaginal penetration
- Difficulty achieving vaginal penetration
- Feeling that there is a block preventing vaginal penetration
- Discomfort and difficulty when having a vaginal examination or smear test
- Anxiety around penetrative sex/vaginal penetration
What Causes Vaginismus?
The causes of vaginismus are not always obvious. There can be a mixture of biological, social, cultural and psychological factors involved, for example:
- An underlying physical condition, such as thrush or a skin condition, may trigger pain during sex and over time this might lead to the development of vaginismus.
- Beliefs, anxieties or fears surrounding sex may play a part. A fear of penetration, a belief that it will be painful, or a fear of sexually transmitted infection, or pregnancy, may lead to vaginismus symptoms.
- Some women may develop vaginismus as a result of a negative experience, for example sexual assault, unwanted sex, or a bad/painful experience during a medical examination.
- Some social and cultural messages about penetrative sex may also contribute to the development of vaginismus.
It isn’t always completely clear-cut and you may not be able to identify the exact cause of your symptoms.
Symptoms of vaginismus can persist for a significant length of time if not treated, even if you actively wish to engage in penetrative activities and even if you had an infection that has now resolved. The muscle spasms are an involuntary reflex response aimed at protecting you from anticipated discomfort - they are not under your conscious control.
Any form of anxiety around penetration can cause the pelvic floor muscles to contract and tighten, making penetration more difficult and in some cases uncomfortable or impossible. This can become a vicious circle in which you anticipate discomfort and your pelvic floor muscles respond by tightening and preventing penetration.
Can Vaginismus be treated?
Yes – vaginismus can be treated. If you think you may have vaginismus you should visit your GP. They may need to do a vaginal examination to rule out infection or any other contributing factors. Depending on the likely causes of your symptoms, your GP may refer you for pelvic health physiotherapy and/or psychosexual therapy. Both of these can help with your symptoms.
You can also refer yourself to pelvic health physiotherapy using the flowing link Pelvic Health Physiotherapy Self-Referral Form
How is Vaginismus Treated?
Treatment usually focuses on managing your feelings around vaginal penetration and exercises to gradually get you used to vaginal penetration.
Treatments may include:
- Mindfulness, breathing techniques, and gentle touch exercises to help you relax your pelvic floor muscles
- Practising techniques that help to release tension in the pelvic floor muscles – see the Pain with Sexual Intercourse section of this website for more information on this.
- Sensate focus – progressive exercises you can work on with your partner to help you relax during sexual activity
- Vaginal trainers – smooth, tampon-shaped devices, of progressively increasing size, that you insert in to your vagina, completely within your comfort level
- Psychosexual therapy – talking therapy that can help you understand and manage your feelings and thoughts about your body and sex
What Can I Do to Help Ease my Symptoms?
It is a good idea to stop the activity that is triggering the vaginismus until you have undergone a course of treatment. Continuing to try to have penetrative sex or use tampons for example, when experiencing vaginismus, can exacerbate the symptoms and be detrimental to your progress.
Useful links
Menopausal symptoms can influence pelvic floor dysfunction symptoms. See below for some useful information regarding the menopause:
 OAK Menopause
OAK Menopause
There are education sessions run to better understand the menopause. You must be registered with a GP within Gwent to access these sessions.
If you would like to register your interest or find out more about the upcoming sessions
Contact methods
- OAK Menopause : 01495 768645
- OAKReferrals.ABB@wales.nhs.uk
Information and fact sheets about menopause are available from:
- Womens Health Concern
- Rock My Menopause
- Menopause Matters
- Menopause
- Diet During the Menopause - Association of UK Dietetics
- Menopause Matters UK
- Vaginal Dryness
- HRT
- Alternatives to HRT
Information for women diagnosed with premature ovarian insufficiency:
You may be referred to Physiotherapy prior to urogynaecology or gynaecology surgery
This is to ensure that your pelvic floor muscles are working to their best ability so they can help to support the surgery being completed.
It may be that you are referred to physiotherapy post surgery
This booklet gives further advice that may aid your recovery following gynaecological surgery
Aneurin Bevan University Health Board and partners have developed the ‘melo’ website to look after the mental wellbeing of its residents. Melo can help you to develop new skills that will support you when life is difficult.

Melo Cymru - Mental Wellbeing Resources, Courses + Advice Gwent Wales
Maintaining a healthy weight can help to alleviate bladder leakage symptoms

Weight Management Service - Aneurin Bevan University Health Board (nhs.wales)

Stopping Smoking can help to alleviate bladder leakage by reducing coughing associated with smoking - Help Me Quit
Exercise

Domestic abuse is not acceptable; anyone experiencing domestic violence and abuse is not to blame and is not alone. Help and support is available.
You may find further information on the below websites and apps
- Bladder Health UK
- Bladder and Bowel Community
- CONfidence App
- Squeezy (squeezyapp.com)
- Patient Information | POGP (thepogp.co.uk)
- yourpelvicfloor.org/leaflet